
Student Case Study
Submitted by Ashley Cubb, Texas A&M University
INVESTIGATION OF OPHTHALMIC LESIONS FROM TRAUMATIC INJURY IN RAPTORS
Ashley Cubb, Erin M. Scott, VMD, DACVO, Sharman M. Hoppes, DVM, DABVP (Avian)
Department of Small Animal Clinical Sciences, College of Veterinary Medicine & Biomedical Sciences, Texas A&M University, College Station, Texas
I. Abstract:
Purpose: To describe the clinical ophthalmic findings and outcome of raptors presented for veterinary evaluation with traumatic injury.
Methods: Medical records of free-living raptors presented to the Texas A&M Veterinary Medical Teaching Hospital (2016-2019) with known or suspected blunt or penetrating trauma that received a complete ophthalmic examination were reviewed.
Results: Twenty-four cases were included comprising 14 owls (7 juveniles, 7 adults), 9 hawks (3 juveniles, 6 adults), and 1 adult eagle. Blunt trauma was the most common cause of injury in 21/24 cases. Ocular lesions were detected in 21/24 birds with 14/21 affected bilaterally and 7/21 affected unilaterally. The most common ophthalmic findings included traumatic uveitis, retinal tears, cataracts, corneal abrasions, and cyclodialysis. Most cases retained vision in at least one eye (23/24) and were discharged to a rehabilitation center (19/24), with only 5/24 euthanized prior to rehabilitation for the extent of their ocular and nonocular injuries.
Conclusion: A full ophthalmic evaluation in raptors is crucial to assess ocular morbidity and visual prognosis to ultimately determine eligibility for future release.
Keywords: Eye, ophthalmology, avian, raptor, trauma
II. Introduction:
Raptors are known for high-functioning visual acuity that is necessary for survival. However, many features that enhance avian vision, such as large eye size, also predispose them to injury. In free-living raptors, ocular abnormalities are primarily attributed to traumatic injury (Carter et al 2021). Injury to the eye may impair vision, and therefore, affect the bird’s potential for release. Studies have shown that up to 28% of raptors presented to rehabilitation facilities have at least one ocular lesion (Murphy 1982). Raptors that have significant bilateral ocular lesions are not considered releasable, as they rely heavily on their visual acuity to locate prey and avoid predators. The ability to release raptors with severe vision-altering lesions in only one eye is a controversial topic. However, there is an agreement that factors such as the type of ocular injury, age, size, and species of the patient must play a role when deciding eligibility for future release (Redig et al 2007).
A complete ophthalmic examination along with a comprehensive evaluation of overall health is vital to determining the visual prognosis and suitability for release of injured raptors. However, assessing vision of in birds of prey is challenging in several regards. Many raptor species are known to be stoic in nature, making it difficult to assess pain and response to visual stimuli. In addition, systemic disease, head injury, or both may affect their mental status and complicate visual assessments. For this reason, before performing an ophthalmic examination the patient should receive a physical examination to identify signs of injury and ensure the patient is in the appropriate mental and physical condition to tolerate the stress of additional restraint (Labelle. 2011). Once the bird is systemically stable, the proper identification and treatment of ocular lesions caused by trauma aids in determining eligibility for rehabilitation and release of free-living raptors. The purpose of this study was to describe the clinical ophthalmic findings and outcome of raptors presented for evaluation to a veterinary teaching hospital with traumatic injury.
III. Materials and methods:
Medical records of free-living raptors that were presented to the Zoological Medicine Service at Texas A&M Veterinary Medical Teaching Hospital (TAMU-VMTH) from 2016 to 2019 for trauma were reviewed. Clinical information and follow-up were obtained from a rehabilitation center when available. Inclusion criteria required cases with a known or suspected history of blunt or penetrating trauma that received a complete ophthalmic examination and consultation by the Comparative Ophthalmology Service. Information retrieved from the patient record included species, estimated age, presenting complaint, eye(s) affected, date and season of presentation, ophthalmic exam findings, medical therapy instituted, and outcome (if known).
All birds were manually restrained in an upright position with their head stabilized to protect the examiner from injury. Intravenous sedation with butorphanol tartrate (1 mg/kg IM, VetOne, Boise, ID, USA) and midazolam hydrochloride (1 mg/kg IM, Athenex, Schaumburg, IL, USA) was administered at the discretion of the Zoological Medicine Service. A complete ophthalmic examination was defined as an evaluation of the ocular adnexa, neuro-ophthalmic assessment, observation of the anterior and posterior segments of the globe, and baseline diagnostic testing. This included slit-lamp biomicroscopy (Kowa SL-17, Kowa, Torrance, CA, USA), indirect ophthalmoscopy (Vantage Plus Wireless Headset, Keeler Instruments, Malvern, PA, USA; 28 or 60 D condensing lens, Volk Optical Inc., Mentor, OH, USA) fluorescein staining (BioGlo, HUB Pharmaceuticals, Plymouth, MI, USA), and rebound tonometry (Tonovet, Icare, Vantaa, Finland). Additional diagnostics, such as B mode ocular ultrasound (VuMax, Sonomed Escalon, Lake Success, NY, USA) examination, were performed as indicated based on the severity of ocular lesions and ability to visualize the posterior segment of the globe. Descriptive data analysis was performed.
IV. Results:
From 2016 – 2019, 24 free-living raptor cases met the selection criteria, comprising 14 owls (7 juveniles, 7 adults), 9 hawks (3 juveniles, 6 adults), and 1 adult eagle (Table 1). A known traumatic event was witnessed in 6/24 cases and highly suspected in 18/24 cases due to the nature in which the birds were found by good Samaritans (i.e., on the side of the road). The ophthalmic lesions identified were consistent with blunt ocular trauma in 21/24 cases and penetrating ocular trauma in 3/24 cases. Nine of 24 cases were presented in the spring (March – May), 5/24 in the summer (June – August), 5/24 in the fall (September – November), and 5/24 in the winter months (December – February).
Ocular lesions were detected in 21/24 birds with 14/21 affected bilaterally and 7/21 affected unilaterally. The most common ophthalmic findings included traumatic uveitis (13/21; Figure 1), corneal abrasions or lacerations (6/21; Figure 2A), cataracts (5/21; Figure 2B), and cyclodialysis (5/21; Figure 3). Other findings included retinal tears (3/21), retinal lenticular metaplasia (3/21), retinal detachment (1/21), retinal hemorrhage (1/21), lens capsule rupture (1/21), and lens subluxation (1/21).
All cases were administered a systemic non-steroidal anti-inflammatory drug (NSAID) (0.5 – 1 mg/kg meloxicam; Boehringer Ingelheim Vetmedica, St. Joseph, MO, USA) to address pain and inflammation associated with both ocular and non-ocular lesions. Systemic antimicrobials were administered to 16/24 raptors to address non-ocular comorbidities. Regarding topical ophthalmic medications, severe traumatic uveitis (>2/4+ aqueous flare with hypopyon) was treated with a topical corticosteroids 4-6 times daily (1% Prednisolone acetate, Sandoz, Trenton, NJ, USA). Moderate to mild cases of traumatic uveitis ( 2/4+ aqueous flare) were administered a topical NSAID 1-2 times daily (0.03% Flurbiprofen, Bausch & Lomb, Bridgewater, NJ, USA). Corneal abrasions and ulcerations were treated with a topical antibiotic 3-4 times daily such as 0.3 % ofloxacin (Akorn, Lake Forest, IL, USA), 0.3% ciprofloxacin (Sandoz, Trenton, NJ, USA), or neomycin-polymyxin B-bacitracin (Bausch & Lomb, Bridegwater, NJ, USA).
Most cases retained vision in at least one eye (23/24) and were discharged to a rehabilitation center (19/24), with only 5/24 euthanized at TAMU-VMTH for the extent of their ocular and non-ocular injuries. Based on further follow up from the rehabilitation center, 6/19 that were discharged for rehabilitation were confirmed to be released. Unfortunately, 7/19 of the remaining raptors that were discharged to the rehabilitation were euthanized. Information regarding the outcome of the remaining 5/19 raptors is currently unknown.
V. Discussion:
Based on the cases reviewed, ocular lesions were a common finding in raptors that presented for trauma. In general, ocular lesions in raptors can be caused by penetrating trauma, blunt trauma, or thermal-type injury (Davidson 1997). From this study, the most common type of trauma was determined to be blunt trauma. There were no cases of thermal-type injury. Moore et al. (2017) described a similar frequency of blunt trauma in avian patients with histological slides of ocular samples reviewed by the Comparative Ocular Pathology Laboratory of Wisconsin. The study also identified that the most frequent lesions found on ocular histopathology were localized to the retina (91% of cases) and iris/ciliary body (77% of cases) (Moore et al 2017). The prevalence of retinal and iris/ciliary body lesions were also noted in the case distribution seen at TAMU-VMTH. In the raptor cases reviewed, 4/21 patients had retinal injury such as retinal tears or retinal detachment. Three of 21 raptors were noted to have acquired lenticular metaplasia which is considered a sign of chronic retinal injury where scar tissue resembling the lens forms within regions of damaged retina (Dubielzig & Zeiss 2005). Injury to the iris/ciliary body was represented as the common finding of cyclodialysis. Cyclodialysis is a sequala of blunt ocular trauma, where a blunt force disrupts the integrity of attachments between the anterior uvea and the sclera. As a result, the iris base and ciliary body are pulled away from the sclera leading to iridocorneal angle recession or iridocyclodialysis (Moore et al 2017).
In this study, owls represented 14/24 or approximately 58% of cases that were reviewed. These results are supported by previous studies which reported that owls may be more prone to ocular injury than other raptors (Moore et al 2017; Murphy et al 1982). Owls have distinct anatomic features that may explain this predilection for ocular injury. For example, owls have flat faces with more frontally positioned eyes along with a large globe: orbit ratio that limits the presence of extraocular muscles or soft tissues that could offer cushion to trauma (Moore et al 2017).
Species differences among raptor should be considered when discussing the impact of visual impairment. For example, while owls have been noted to be more prone to ocular injury, there is some evidence that owls rely less on binocular vision and more on hearing than hawk species (Redig et al 2007). Characteristics regarding predation and use of vision can be attributed to this difference. However, further research will need to be done to determine the ultimate success of raptors released with visual impairment in one eye.
The distinction between diurnal and nocturnal raptors has been reported to play a significant role in both the age and frequency of patients with ocular injury (Hernandez et al 2018). In the study conducted, a predilection for nocturnal raptors, such as owls, was seen. Additionally, there was an equal amount of juvenile and adult owls that were admitted. In contrast, diurnal raptors, such as hawks and eagles, were admitted less frequently in this study with almost twice the number of adult hawks compared to juveniles. In a study performed by Carter et al (2021), adult owls admitted for ocular trauma outnumbered juvenile owls, and juvenile hawks with ocular trauma outnumbered adult hawks. This discrepancy of trends could be due to a relatively small sample size in both studies. Further research should be conducted evaluating the impact that diurnal versus nocturnal behavior may have on ocular injury.
Overall, this study provided further characterization of ophthalmic findings in raptors with trauma and paired these findings with their clinical outcomes and eligibility for rehabilitation. The successful release rate of raptors in the current study with a known outcome was 6/18 or approximately 33%. In conclusion, the effects of ocular injury can be a determining factor in the potential for release of raptors.
Acknowledgements: The authors thank Jennifer Perkins, LVT and Shelby Basey, LVT for their technical assistance.
Literature cited:
Carter, R., and A. Lewin. 2021. Ophthalmic evaluation of raptors suffering from ocular trauma. Journal of Avian Medicine and Surgery. 35(1): 2-27.
Davidson, M. 1997. Ocular consequences of trauma in raptors. Seminars in Avian and Exotic Pet Medicine. 6(3): 121-130.
Dubielzig, R.R., and C.J. Zeiss. 2005. Acquired lenticular metaplasia of Muller cells in the damaged avian retina. Investigative Ophthalmology & Visual Science. 46: 3194.
Hernandez, C. and S. Oster. 2018. Retrospective study of raptors treated at the Southeastern Raptor Center in Auburn, Alabama. Journal of Raptor Research. 52(3): 379-388.
Labelle, A. 2011. Clinical utility of a complete diagnostic protocol for the ocular evaluation of free-living raptors. Veterinary Ophthalmology. 15(1): 5-17.
Moore, B. 2017. The consequences of avian ocular trauma: histopathological evidence and implications of acute and chronic disease. Veterinary Ophthalmology. 20(6): 496-504.
Murphy, CJ. 1982. Ocular lesions in free-living raptors. Journal of the American Veterinary Medical Association. 181(11): 1302-1304.
Redig, P., and G. Klauss. 2007. Clinical techniques: considerations for release of raptors with ocular disease. Journal of Exotic Pet Medicine. 16(2): 101-103
Figure Legends:
Figure 1. (A) Juvenile screech owl with moderate blepharospasm of the right eye from traumatic uveitis. Trace aqueous flare was detected on slit lamp biomicroscopy. (B) Juvenile screech owl with severe uveitis characterized by 4/4+ aqueous flare with hypopyon and fibrin in the anterior chamber. Images courtesy of Lucien Vallone, DVM, DACVO.

Figure 2. (A) Adult owl of unspecified species with a linear, horizontal corneal laceration and adjacent corneal edema in the left eye. This bird was found tangled in a barbed-wire fence. (B) Adult owl of unspecified species with a deep anterior chamber due to a hypermature cataract. Note the pigment from previous posterior synechia on the anterior lens capsule (asterisk). Images courtesy of Lucien Vallone, DVM, DACVO.
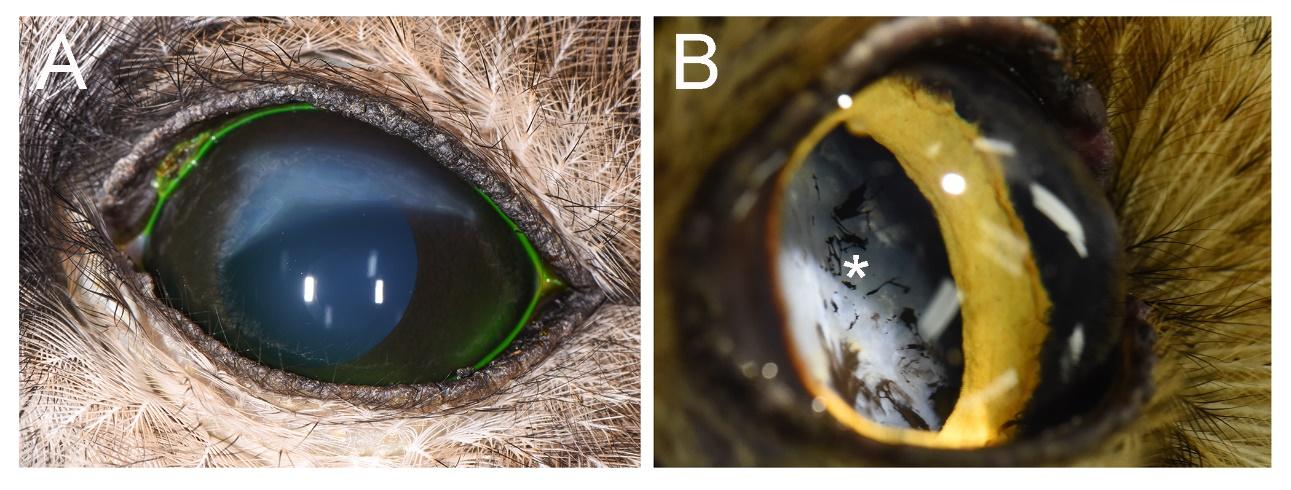
Figure 3. (A) Normal right eye of a juvenile red-tailed hawk. (B) Left eye of the same bird with mild traumatic uveitis characterized by trace aqueous flare and cyclodialysis (asterisks). Images courtesy of Lucien Vallone, DVM, DACVO.

 Share this Post | Comments Off
Share this Post | Comments Off